

Adverse Childhood Experiences, Dysfunctional Households, and Circumcision
 Shutterstock/Superstar
Shutterstock/Superstar
Abstract: Children from dysfunctional households experience a proportionally greater number of adverse experiences than other children. One such common event is male child genital cutting, or circumcision. This study surveyed five-hundred randomly selected circumcised and intact men concerning their experiences before 18 years of age using the 10- item Adverse Childhood Experiences checklist (ACE). The cumulative scores for men with circumcised penises (2.83) were higher on average compared to those for men with intact penises (2.44). In this cohort, male child genital cutting was more common in dysfunctional, violent households.
Introduction
Dysfunctional households, defined in this study as a family system in which a child experiences four or more ACEs, have a tremendous influence on the health and welfare of children, including higher ACE results. Among other lifelong health issues, higher ACE results indicate reduced emotional intelligence (Priyam & Nath, 2021), a two-fold increase in baseline PTSD scores (Boyle & Ramos, 2019), increased risk of suicide (Dube et al., 2001), addiction (Felitti et al., 1998), and shorter lifespans (Grummitt et al., 2021). Crenshaw et al. (2021) recommended screening for ACEs in one-year-old children, which underscores the possibility of acquiring ACEs at an early age. The ACEs checklist identifies dysfunctional households and records the specific traumas an individual child experienced within that household. This study correlates ACEs checklist and circumcision status.
An estimated 1.4 million parents in the United States consent to having their newborn sons undergo male child genital cutting (MCGC) annually (Intact America, 2020). Parents’ reasons for choosing MCGC vary greatly (Gollaher, 1994). Some studies have concluded that the dominant deciding factor is the mother’s preference (Dyal, 2006) or the father’s penile status (Spense et al., 2017). Hygiene is a commonly stated reason (Tiemstra, 1999). Some parents believe that circumcision is an eventuality, so they might as well do it in infancy to prevent him from remembering the pain (Lunde et al., 2020). Health concerns in general (Guevara et al., 2021), HIV (Kline et al., 2010) and UTI risk (Turini III et al., 2004) are also reasons that parents give, even though such claims have been refuted (Van Howe, 2013). Other deciding factors include the cultural norm (Dyal, 2006), race (Spense et al., 2017), and parental education (Binner et al., 2002). Sociocultural factors also influence the parental decision-making process (Morgan et al., 2021). However, elective MCGC is medically non-indicated, according to the American Academy of Pediatrics Task Force on Circumcision (2012), and no medical society in the world recommends this prophylactic surgery.
It is not known if environmental factors, such as being born into a dysfunctional household, influence the MCGC decision. The long-term effects of MCGC have not been methodically studied, according to Tye and Sardi (2022), and no study has investigated the association between MCGC and ACEs to date. This study focuses on the MCGC prevalence in dysfunctional households as measured by participants’ ACE scores.
Materials and Methods
Five hundred men between 18 and 45 years of age were surveyed in the United States. Participants were divided into two groups, Men with Circumcised Penises (MCP, n = 375) and Men with Intact Penises (MIP, n = 125). Participants completed a modified 10-item ACEs checklist. The two modifications were: 1) they were instructed not to include their circumcision in Question #3, assessing sexual abuse, and 2) Question #7, asking about witnessing violence in the household, was changed by replacing the terms ‘mother or stepmother’ with ‘caregiver.’
Qualtrics Online Sample research team, Provo, Utah, conducted a national, random-sample survey for this study. Participants provided Qualtrics, Inc. written consent to participate in their online research panels. Participants were advised in advance that this survey would ask about traumatic experiences they might have had and that they could opt out before taking the survey or at any time during the survey. The data were analyzed using Qualtrics’ integrated reports and Microsoft Excel 365 Data Analysis Tool pack.
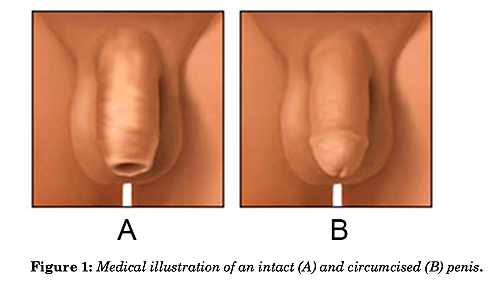
Risser et al. (2004) found that about one-third of young men are mistaken or unsure whether they are circumcised or intact. Therefore, circumcision status was verified using a novel two-factor method by asking whether they were circumcised or intact and then matching their answer with the correct color illustration of a circumcised or intact penis, as seen in Figure 1. Only validated entries were accepted for inclusion in the study.
Results
ACE scores varied by penile status. Scores for MCP were higher for nine checklist items compared to those for MIP except for Question #6 regarding divorce, as seen in Table 1 (appendix). The cumulative ACE score for all 500 participants in this study was 2.73 (SD = 2.80, 95% CL = 0.25). ACE scores for MCP were 0.39 points higher compared to those for MIP (p = .08), specifically, 2.83 for MCP (SD = 2.88, 95% CL = 0.29) and 2.44 for MIP (SD = 2.55, 95% CL = 0.45).
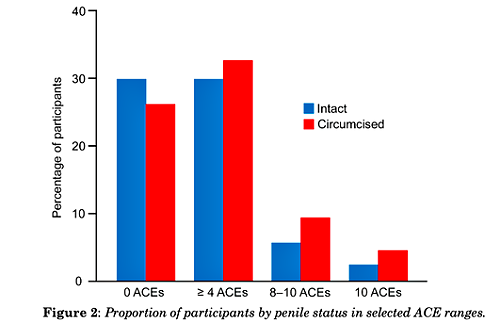
A greater percentage of MCP had higher ACE scores across the 0–10 range of possible ACE scores compared to MIP, except for zero ACEs. MCP (25.9%) were 17% less likely (OR = 0.83) to have zero ACEs compared to MCP (29.6%). For ACE scores of one and higher, MCP (74.1%) were 21% more likely to have higher scores (OR = 1.21) versus MIP (70.4%).
The percentages of participants (and the odds ratios) for those from dysfunctional households (having four or more ACEs) were higher for MCP than for MIP. Regarding participants with ACE scores of four and higher, MCP (32.3%, avg. 6.42, SD = 2.01, 95% CL = 0.36) were 13% more likely to have higher scores (OR = 1.13, p = .04) than MIP (29.6%, avg. 5.78, SD = 1.83, 95% CL = 0.61), and with a difference of 0.64 points. For ACE scores 8 and higher (9.3% versus 5.6%), the odds ratio was almost double (OR = 1.74). Additionally, a total score of ten ACEs (4.5% versus 2.4%) was double (OR = 1.93) for MCP, as shown in Figure 2.
Unloved and Alone
MCP were 38% more likely to report in Question #4 that they felt “unloved” and “unimportant” in the household (OR = 1.38, p = .08). And MCP were 50% more likely to report in Question #9 that a family member attempted suicide (OR = 1.50, p = .04).
Violence and Abuse
Scores for Question #7 regarding witnessing violence, such as a caregiver being pushed, grabbed, slapped, or threatened with a knife or gun, were significantly associated with MCGC (p = .008). MCP (0.18 avg., SD = 0.38, 95% CL = 0.04) were twice as likely to witness violence (OR = 2.01) compared to MIP (0.10 avg., SD = 0.30, 95% CL = 0.05).
Aggregate ACE scores for the four questions involving violence and abuse were almost three times higher (OR = 2.77) for MCP (1.22 avg., SD = 1.38, 95% CL = 0.14) than for MIP (0.98 avg., SD = 1.18, 95% CL = 0.21) (p = .04). Those questions concerned: fear of violence (#1), experienced injury and corporal punishment (#2), witnessed physical assault (#7), and witnessed household mental illness or attempted suicide (#9).
Discussion
ACEs encompass ten subcategories of childhood adversity developed by the Centers for Disease Control & Prevention (CDC) for their Adverse Childhood Experiences Study (Felitti et al., 1998). The checklist included three types of abuse (emotional, physical, sexual), five types of household challenges (household partner violence, household substance abuse, mental illness in the household, loss of a parent due to parental death, separation, or divorce, incarceration of a family member), and two types of neglect (emotional, physical).
Psychological harm from MCGC has been discussed by researchers for more than fifty years commencing with Cansever (1965). No study during that timeframe has concluded that childhood circumcision is beneficial to the boy’s psyche (Bollinger, 2014). However, limited research has produced measurable results regarding the psychological, psychosocial, and psychosexual aspects of penile circumcision (Tye & Sardi, 2022). Boyle et al. (2002) found that MCGC is a frequent, early, and painful psychosexual trauma. Regardless of what anesthesia is administered, the newborn experiences clinically significant pain (Bellieni, 2022). MCGC has been linked to alexithymia, the inability to identify and express emotions (Bollinger & Van Howe, 2011), and is associated with multiple altered adult socio-affective processing (Miani et al., 2020).
ACEs’ Effects
A graded dose-response relationship has been observed between cumulative ACE scores (Hambrick et al., 2019) and the likelihood of moderate to heavy drinking, drug use, depressed affect, and suicide attempts in adulthood (Merrick et al., 2017). ACE scores of 4 or more is a de facto critical threshold (Briggs et al., 2021), resulting in a substantial increase in at-risk health consequences (Central Iowa ACEs Steering Committee, 2012), a seven-fold increase in alcoholism, a two-fold increase in cancer risk (Felitti et al., 1998), and a 32-fold increase in learning/behavior problems and obesity (Burke et al., 2011). Childhood trauma (Jiang et al., 2019) and toxic stress damage the structure and function of the developing brain (de Magalhães-Barbosa et al., 2022; Dunn et al., 2019), and are associated with long-lasting epigenetic changes (Bearer & Mulligan, 2018).
Parental neglect increases children’s ACEs (Priyam & Nath, 2021). Parent-child aggression can have long-term effects on behavior (Maneta et al., 2017). Mothers with higher ACE scores can negatively affect their children’s development (Riggs et al., 2021), affecting the next generation through epigenetic responses (Folger et al., 2022), including age acceleration (Nwanaji-Enwerem et al., 2021). Such mothers are more likely to have children with behavioral (Schickedanz et al., 2018) and mental health problems (Kang et al., 2021).
McKelvey et al. (2017) mention that non-explicit adverse experiences (those not listed in the original ACE checklist) also put the children at risk for poorer physical health and early development and should be given due consideration for inclusion into the checklist.
MCGC as an ACE
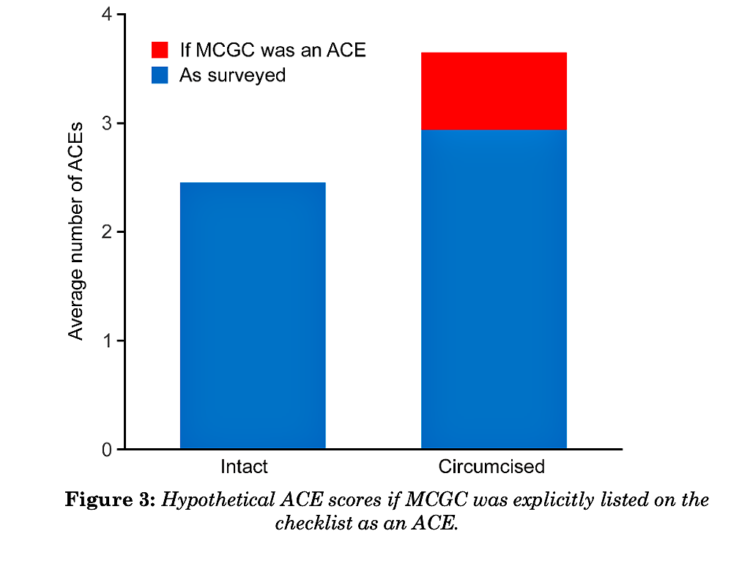
Participants were asked in the survey not to include their circumcision when answering Question #3, assessing sexual abuse. But what if the ACE checklist had explicitly mentioned circumcision in that question? To investigate, “No” answers for MCP were temporarily changed to “Yes.” The ACE scores for Question #3 would then be one hundred percent for MCP (while MIP scores remained unchanged at 18%). Subsequently, the average cumulative ACE scores for all ten questions on the checklist for MCP would increase from 2.93 to 3.63, resulting in 1.19 more ACEs for MCP compared to MIP (p < .001), as shown in Figure 3.
Implications
The survey results indicate that MCGC is associated with dysfunctional households and may qualify as an ACE. Adding childhood genital cutting (including male and female circumcision and intersex gender-norming surgery) would better capture these common early traumas (Bollinger & Chapin, 2019), which suggested adding: “…or surgically alter your genitals or circumcise you at birth or later?” to Question #3. An ACEs quiz that includes this addition to the current 10- item ACEs checklist is available online (Intact America, n.d.).
Spanking, another form of parent-child violence, has been proposed as an ACE, too (Afifi et al., 2017).
Conclusion
In this cohort, MCP were 1.21 times more likely to come from dysfunctional households. MCP had aggregate ACE scores a half-point higher on average compared to MIP. That difference would increase to 1.19 points if MCGC were explicitly included by researchers as an ACE in the checklist. MCP had higher scores for nine of the ten checklist items compared to MIP. MCP also had much higher scores and odds for four or more ACEs. MCGC is more common and strongly associated with violent, suicidal, and unloving households. Further research is indicated regarding MCGC as an early trauma. Incorporating child genital cutting to the ACEs checklist may be advisable following validation of the suggested addition to Question #3 of the checklist.
Publication Citation: Journal for Prenatal and Perinatal Psychology and Health, 36(3), Fall 2022, pp 76–87.
Kindred Resources
Kindred articles and videos on on ACES and Trauma Recovery
Kindred Circumcision Resources
Kindred Circumcision Posts, Videos, Podcasts